

Volume 31, Issue 2 (7-2022)
JGUMS 2022, 31(2): 150-165 |
Back to browse issues page



Research code: 94063103
Ethics code: IR.GUMS.REC.1394.263
![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Soltani Moghadam R, Azaripour E, Akbari M, Behboudi H, Mohammad Amin H. Predicting the Keratoconus Disease Severity Based on Pachymetric Progression Indices Measured by Pentacam. JGUMS 2022; 31 (2) :150-165
URL: http://journal.gums.ac.ir/article-1-2452-en.html
URL: http://journal.gums.ac.ir/article-1-2452-en.html
Reza Soltani Moghadam1 

 , Ebrahim Azaripour * 2, Mitra Akbari3 , Hassan Behboudi3 , Homafar Mohammad Amin3
, Ebrahim Azaripour * 2, Mitra Akbari3 , Hassan Behboudi3 , Homafar Mohammad Amin3
, Ebrahim Azaripour * 2, Mitra Akbari3 , Hassan Behboudi3 , Homafar Mohammad Amin3
1- Department of Eye, Eye Research Center, Amiralmomen in Hospital, Faculty of Medicine, Guilan University of Medical Science, Rasht, Iran.
2- Department of Eye, Eye Research Center, Amiralmomenin Hospital, Faculty of Medicine, Guilan University of Medical Science, Rasht, Iran. , eazaripour@yahoo.com
3- Department of Eye, Eye Research Center, Amiralmomenin Hospital, Faculty of Medicine, Guilan University of Medical Science, Rasht, Iran.
2- Department of Eye, Eye Research Center, Amiralmomenin Hospital, Faculty of Medicine, Guilan University of Medical Science, Rasht, Iran. , eazaripour@yahoo.com
3- Department of Eye, Eye Research Center, Amiralmomenin Hospital, Faculty of Medicine, Guilan University of Medical Science, Rasht, Iran.
Full-Text [PDF 5276 kb]
(262 Downloads)
| Abstract (HTML) (802 Views)
References
Full-Text: (276 Views)
Introduction
keratoconus (KCN) is a common disorder in ophthalmology. It characterized by thinning and protrusion of central and paracentral areas of the cornea such that the cornea turn into a conical shape in the advance stage of the disease [1, 2]. A systematic review conducted in 1998 estimated the prevalence of KCN between 0.05% and 0.23%. The disease is less common in Asian countries than in European countries. The prevalence of KCN is considerable in Iran but no epidemiological study has been conducted so far [3]. The onset of KCN is during puberty and its progress continues until the 3rd and 4th decades of life. The inheritance pattern of the disease is not prominent and predictable, but a positive family history has been reported in 6-8% of cases. The combination of genetic and environmental risk factors such as eye rubbing and inflammation and oxidative stress all play a role in the onset and progression of KCN.
The severity of KCN disease is important for accurate and timely treatment of patients. Although the classic classification standard of KCN severity is the Amsler-krumeich classification, due to the creation of new imaging indicators in recent years, other standard such as High-order Aberration have been proposed to classify KCN [8]. This study aims to determine whether the pachymetric progression indices (PPIs) can be used to grade the severity of KCN disease.
Methods
This cross-sectional study was performed in Amir Al-Momenin Hospital in Rasht, Iran in 2014-2015. Data collected from 76 patients with definitive diagnosis of KCN who had at least one of the specific symptoms of KCN (Flasher’s ring, Vogt striae, anterior stromal scar, stromal thinning, conical protrusion in symmetrical apex, etc.), examined by a slit lamp or had topographic findings characterizing KCN. Individuals aged <12 years with a history of systemic disease, previous corneal or intraocular surgery, history of chemical damage or delayed corneal epithelial repair, neuropathology, pregnancy and lactation were excluded.
Descriptive statistics (frequency, mean, and standard deviation) were used to describe demographic characteristics (age, gender), affected eye, and KCN disease severity. Shapiro-Wilk test was used to determine the normality of data distribution. Spearman correlation test was used to determine the correlation, and independent t-test, Mann-Whitney U and Kruskal-Wallis tests were used to determine and compare KCN severity and PPIs in IBM SPSS v.21 software. The data were quality checked by Pentacam and the appropriate data were selected. The significance level was set at 0.05. The receiver operating characteristic (ROC) curve was used to assess the severity of KCN based on PPIs.
Results
Participants were 76 patients with KCN; 69% (n= 53) were male and 30% (n=23) were female, with a mean age of 25.5 ± 6.8 years, ranged from 15 to 47 years. The results showed that 52% (n=40) had KCN in the right eye and 47% (n=36) had KCN in the left eye. In terms of KCN severity, 18% of cases were at grade 1, 31% at grade 2, 42% at grade 3, and 7% at grade 4. The KCN severity had a significant correlation with PPI Max (r=0.761, P<0.001), PPI Mean (r=0.733, P<0.001), and PPI Ave (r=0.774, P<0.001) (Table 1).
.jpg)
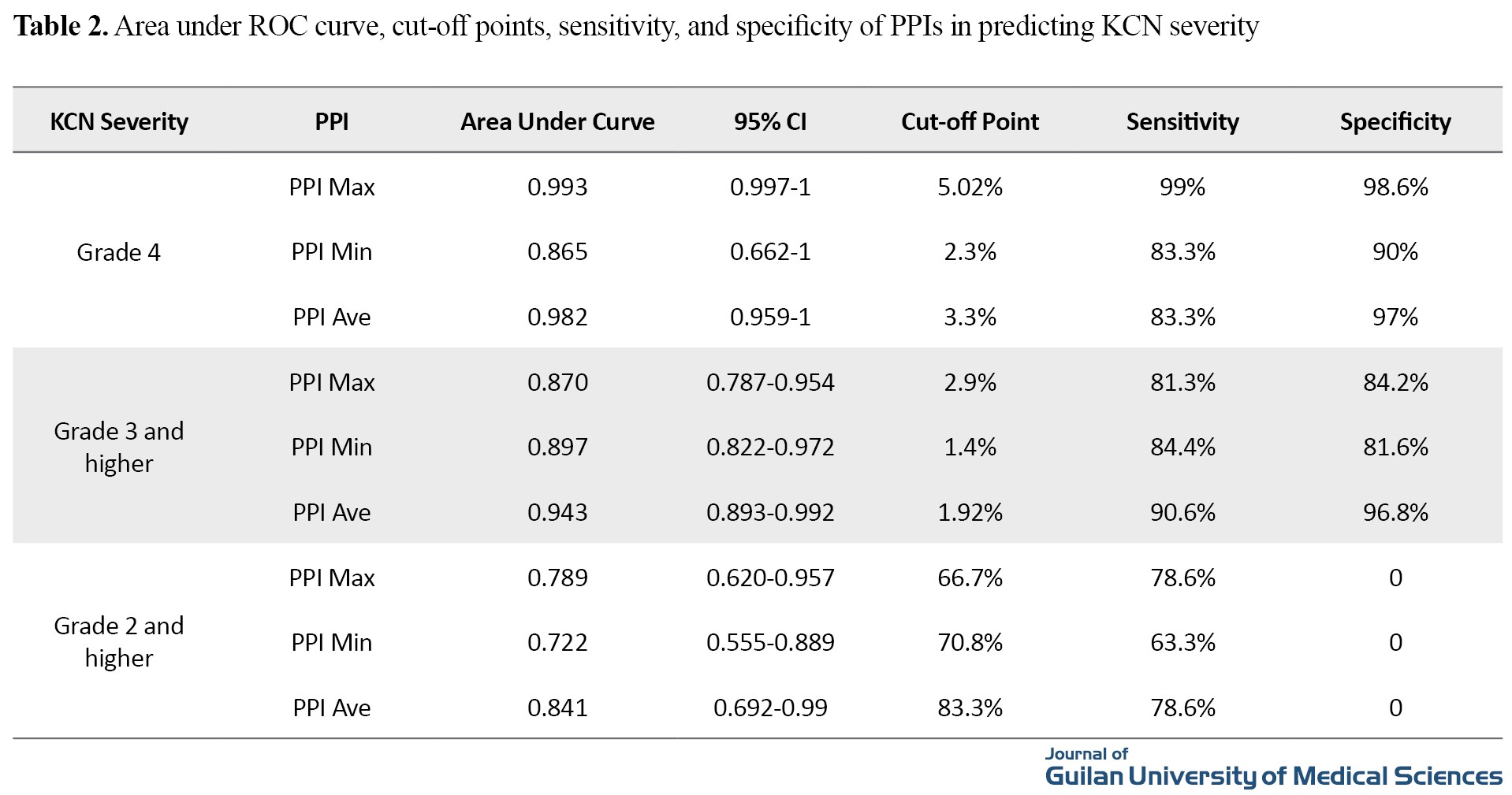
PPI Max, PPI Min and PPI Ave values indicated that the power of PPIs (area under the curve) for predicting the KCN grade 4 was statistically significant and equal to 0.993, 0.865 and 0.982, respectively (P<0.001). The best cutoff point for detection of KCN grade 4 in PPI Max was 5.02 with 99% sensitivity and 98.6% specificity; for PPI Min, it was 2.3 with 83.3% sensitivity and 90% specificity; and for PPI Ave, it was 3.3 with 83.3% sensitivity and 97% specificity. The power of these indices for predicting the KCN grade 3 and above was also statistically significant and equal to 0.870, 0.897 and 0.943, respectively. The best cut-off point for detecting KCN grade 3 in PPI Max was 2.9 with 81.3% sensitivity and 84.2% specificity; for PPI Min, it was 1.4 with 84.4% sensitivity and 81.6% specificity; and for PPI Ave, it was 1.92 with 90.6% sensitivity and 96.8% specificity (Table 2).
The K-Max and K-Mean indices had moderate and high significant correlation with PPIs in all degrees of KCN, while Thinnest Location indices showed the highest significant correlation with PPIs in KCN grade 3. The astigmatism index had no significant correlation with PPIs. This may be due to the sample size of the groups. Ambrosio Relational Thickness (ART) Max had significant negative correlation with PPIs in all degrees of KCN (P<0.01).
Discussion
KCN is a bilateral, progressive, non-inflammatory lesion of the cornea that results in corneal thinning and protrusion. Studies have classified this disease given that it can now be identified and treated with tools. Most of this classification is based on keratometric criteria, clinical symptoms, KCN symmetry, and pre-KCN. Although the Amsler-Krumeich classification has traditionally been used to classify the severity of KCN, new tools and criteria, including topographic information, have received the attention [5, 6].
The present study showed that K-Max and K-Mean indices had a moderate to high significant positive correlation with PPIs in all degrees of KCN, while Thinnest Location showed the highest significant correlation with PPIs in KCN grade 3. The astigmatism index had no significant relationship with PPIs, may be due to the size of groups.
Another result was the direct significant correlation between PPIs and the severity of KCN. With further increase in PPIs, the severity of KCN also increases. In the study by Lim et al., it was observed that PPIs in the two groups of KCN and healthy eyes were significantly different. However, when they evaluated various factors for diagnostic adaptation of KCN disease based on the area under the ROC curve, the difference between PPIs and ART indices for diagnostic evaluation was not significant [7].
The effect of gender and age were also examined in this study. The results showed that the increase in KCN severity could increase the PPI Max, PPI Min and PPI Ave in both genders, indicating no significant effect of gender. On the other hand, the increase in KCN severity could increase these PPIs significantly in the age groups <25 and >25 years. This indicates that PPIs could determine the severity of KCN, regardless of patients’ age.
In conclusion, PPIs can estimates KCN disease severity, regardless of gender and age of patients, and can be used for determining the severity of KCN.
Ethical Considerations
Compliance with ethical guidelines
This research was approved by the Ethics Committee of Gilan University of Medical Sciences and was conducted in accordance with the principles of the Declaration of the World Medical Association of Helsinki with the code: IR.GUMS.REC.1394.263.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
Conceptualization, study design and data analysis and interpretation: Ebrahim Azaripour and Reza Soltani Moghadam; Drafting of the manuscript: Ebrahim Azaripour, Reza Soltani Moghadam, Hassan Behboudi, Mitra Akbari and Mohammad Amin Humafar; Critical revision of the manuscript for important intellectual content, study supervision and statistical analysis: Ebrahim Azaripour; Attracting financial resources: Reza Soltani Moghadam; Administrative, technical or material support: Ebrahim Azaripour, Reza Soltani Moghadam and Hassan Behboodi.
Conflicts of interest
The authors declare no conflict of interest.
Acknowledgements
The authors would like to thank the experts in the Center for Eye Research including Ghazaleh Mohammadi and all patients who participated in this study
keratoconus (KCN) is a common disorder in ophthalmology. It characterized by thinning and protrusion of central and paracentral areas of the cornea such that the cornea turn into a conical shape in the advance stage of the disease [1, 2]. A systematic review conducted in 1998 estimated the prevalence of KCN between 0.05% and 0.23%. The disease is less common in Asian countries than in European countries. The prevalence of KCN is considerable in Iran but no epidemiological study has been conducted so far [3]. The onset of KCN is during puberty and its progress continues until the 3rd and 4th decades of life. The inheritance pattern of the disease is not prominent and predictable, but a positive family history has been reported in 6-8% of cases. The combination of genetic and environmental risk factors such as eye rubbing and inflammation and oxidative stress all play a role in the onset and progression of KCN.
The severity of KCN disease is important for accurate and timely treatment of patients. Although the classic classification standard of KCN severity is the Amsler-krumeich classification, due to the creation of new imaging indicators in recent years, other standard such as High-order Aberration have been proposed to classify KCN [8]. This study aims to determine whether the pachymetric progression indices (PPIs) can be used to grade the severity of KCN disease.
Methods
This cross-sectional study was performed in Amir Al-Momenin Hospital in Rasht, Iran in 2014-2015. Data collected from 76 patients with definitive diagnosis of KCN who had at least one of the specific symptoms of KCN (Flasher’s ring, Vogt striae, anterior stromal scar, stromal thinning, conical protrusion in symmetrical apex, etc.), examined by a slit lamp or had topographic findings characterizing KCN. Individuals aged <12 years with a history of systemic disease, previous corneal or intraocular surgery, history of chemical damage or delayed corneal epithelial repair, neuropathology, pregnancy and lactation were excluded.
Descriptive statistics (frequency, mean, and standard deviation) were used to describe demographic characteristics (age, gender), affected eye, and KCN disease severity. Shapiro-Wilk test was used to determine the normality of data distribution. Spearman correlation test was used to determine the correlation, and independent t-test, Mann-Whitney U and Kruskal-Wallis tests were used to determine and compare KCN severity and PPIs in IBM SPSS v.21 software. The data were quality checked by Pentacam and the appropriate data were selected. The significance level was set at 0.05. The receiver operating characteristic (ROC) curve was used to assess the severity of KCN based on PPIs.
Results
Participants were 76 patients with KCN; 69% (n= 53) were male and 30% (n=23) were female, with a mean age of 25.5 ± 6.8 years, ranged from 15 to 47 years. The results showed that 52% (n=40) had KCN in the right eye and 47% (n=36) had KCN in the left eye. In terms of KCN severity, 18% of cases were at grade 1, 31% at grade 2, 42% at grade 3, and 7% at grade 4. The KCN severity had a significant correlation with PPI Max (r=0.761, P<0.001), PPI Mean (r=0.733, P<0.001), and PPI Ave (r=0.774, P<0.001) (Table 1).
PPI Max, PPI Min and PPI Ave values indicated that the power of PPIs (area under the curve) for predicting the KCN grade 4 was statistically significant and equal to 0.993, 0.865 and 0.982, respectively (P<0.001). The best cutoff point for detection of KCN grade 4 in PPI Max was 5.02 with 99% sensitivity and 98.6% specificity; for PPI Min, it was 2.3 with 83.3% sensitivity and 90% specificity; and for PPI Ave, it was 3.3 with 83.3% sensitivity and 97% specificity. The power of these indices for predicting the KCN grade 3 and above was also statistically significant and equal to 0.870, 0.897 and 0.943, respectively. The best cut-off point for detecting KCN grade 3 in PPI Max was 2.9 with 81.3% sensitivity and 84.2% specificity; for PPI Min, it was 1.4 with 84.4% sensitivity and 81.6% specificity; and for PPI Ave, it was 1.92 with 90.6% sensitivity and 96.8% specificity (Table 2).
The K-Max and K-Mean indices had moderate and high significant correlation with PPIs in all degrees of KCN, while Thinnest Location indices showed the highest significant correlation with PPIs in KCN grade 3. The astigmatism index had no significant correlation with PPIs. This may be due to the sample size of the groups. Ambrosio Relational Thickness (ART) Max had significant negative correlation with PPIs in all degrees of KCN (P<0.01).
Discussion
KCN is a bilateral, progressive, non-inflammatory lesion of the cornea that results in corneal thinning and protrusion. Studies have classified this disease given that it can now be identified and treated with tools. Most of this classification is based on keratometric criteria, clinical symptoms, KCN symmetry, and pre-KCN. Although the Amsler-Krumeich classification has traditionally been used to classify the severity of KCN, new tools and criteria, including topographic information, have received the attention [5, 6].
The present study showed that K-Max and K-Mean indices had a moderate to high significant positive correlation with PPIs in all degrees of KCN, while Thinnest Location showed the highest significant correlation with PPIs in KCN grade 3. The astigmatism index had no significant relationship with PPIs, may be due to the size of groups.
Another result was the direct significant correlation between PPIs and the severity of KCN. With further increase in PPIs, the severity of KCN also increases. In the study by Lim et al., it was observed that PPIs in the two groups of KCN and healthy eyes were significantly different. However, when they evaluated various factors for diagnostic adaptation of KCN disease based on the area under the ROC curve, the difference between PPIs and ART indices for diagnostic evaluation was not significant [7].
The effect of gender and age were also examined in this study. The results showed that the increase in KCN severity could increase the PPI Max, PPI Min and PPI Ave in both genders, indicating no significant effect of gender. On the other hand, the increase in KCN severity could increase these PPIs significantly in the age groups <25 and >25 years. This indicates that PPIs could determine the severity of KCN, regardless of patients’ age.
In conclusion, PPIs can estimates KCN disease severity, regardless of gender and age of patients, and can be used for determining the severity of KCN.
Ethical Considerations
Compliance with ethical guidelines
This research was approved by the Ethics Committee of Gilan University of Medical Sciences and was conducted in accordance with the principles of the Declaration of the World Medical Association of Helsinki with the code: IR.GUMS.REC.1394.263.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
Conceptualization, study design and data analysis and interpretation: Ebrahim Azaripour and Reza Soltani Moghadam; Drafting of the manuscript: Ebrahim Azaripour, Reza Soltani Moghadam, Hassan Behboudi, Mitra Akbari and Mohammad Amin Humafar; Critical revision of the manuscript for important intellectual content, study supervision and statistical analysis: Ebrahim Azaripour; Attracting financial resources: Reza Soltani Moghadam; Administrative, technical or material support: Ebrahim Azaripour, Reza Soltani Moghadam and Hassan Behboodi.
Conflicts of interest
The authors declare no conflict of interest.
Acknowledgements
The authors would like to thank the experts in the Center for Eye Research including Ghazaleh Mohammadi and all patients who participated in this study
References
- Gordon-Shaag A, Millodot M, Shneor E. The epidemiology and etiology of keratoconus. International Journal of Keratoconus and Ectatic Corneal Diseases. 2012; 1(1)7-15. [DOI: 10.5005/jp-journals-10025-1002]
- Gokhale NS. Epidemiology of keratoconus. Indian Journal Of Ophthalmology. 2013; 61(8):382-3. [DOI:10.4103/0301-4738.116054] [PMID] [PMCID]
- Ziaei H, Jafarinasab M, Javadi M, Katibeh M, Poorsalman H, Karimian F, et al. [Epidemiology of Keratoconus in Yazd Province (Persian)]. 2010; 16 (1):9-18. [Link]
- Holland DR, Maeda N, Hannush SB, Riveroll LH, Green MT, Klyce SD, et al. Unilateral keratoconus: Incidence and quantitative topographic analysis. Ophthalmology. 1997; 104(9):1409-13. [DOI:10.1016/S0161-6420(97)30123-7]
- Lee LR, Hirst LW, Readshaw G. Clinical detection of unilateral keratoconus. Australian and New Zealand Journal of Ophthalmology. 1995; 23(2):129-33. [DOI:10.1111/j.1442-9071.1995.tb00141.x] [PMID]
- Copeman PW. Eczema and keratoconus. British Medical Journal. 1965; 2(5468):977. [DOI:10.1136/bmj.2.5468.977] [PMID] [PMCID]
- Ambrósio R Jr, Caiado AL, Guerra FP, Louzada R, Sinha RA, Luz A, et al. Novel pachymetric parameters based on corneal tomography for diagnosing keratoconus. Journal of Refractive Surgery. 2011; 27(10):753-8. [DOI:10.3928/1081597X-20110721-01] [PMID]
- Belin MW, Ambrósio R Jr. Corneal ectasia risk score: Statistical validity and clinical relevance. Journal of Refractive Surgery. 2010; 26(4):238-40. [DOI:10.3928/1081597X-20100318-01] [PMID]
- Dastjerdi MH, Hashemi H. A quantitative corneal topography index for detection of keratoconus. Journal of Refractive Surgery. 1998; 14(4):427-36. [DOI:10.3928/1081-597X-19980701-09] [PMID]
- Smolek MK, Klyce SD. Current keratoconus detection methods compared with a neural network approach. Investigative Ophthalmology & Visual Science. 1997; 38(11):2290-9. [PMID]
- Muftuoglu O, Ayar O, Ozulken K, Ozyol E, Akıncı A. Posterior corneal elevation and back difference corneal elevation in diagnosing forme fruste keratoconus in the fellow eyes of unilateral keratoconus patients. Journal of Cataract & Refractive Surgery. 2013; 39(9):1348-57. [DOI:10.1016/j.jcrs.2013.03.023] [PMID]
- Lim HB, Tan GS, Lim L, Htoon HM. Comparison of keratometric and pachymetric parameters with Scheimpflug imaging in normal and keratoconic Asian eyes. Clinical Ophthalmology. 2014; 8:2215-20. [DOI:10.2147/OPTH.S66598] [PMID] [PMCID]
- Ambrósio R Jr, Belin MW. Imaging of the cornea: Topography vs tomography. Journal of Refractive Surgery. 2010; 26(11):847-9. [DOI:10.3928/1081597X-20101006-01] [PMID]
- McMahon TT, Szczotka-Flynn L, Barr JT, Anderson RJ, Slaughter ME, Lass JH, et al. A new method for grading the severity of keratoconus: The Keratoconus Severity Score (KSS). Cornea. 2006; 25(7):794-800. [DOI:10.1097/01.ico.0000226359.26678.d1] [PMID]
- Mbrósio R Jr, Caiado AL, Guerra FP, Louzada R, Sinha RA, Luz A, et al. Novel pachymetric parameters based on corneal tomography for diagnosing keratoconus. Journal of Refractive Surgery; 27(10):753-8. [DOI:10.3928/1081597X-20110721-01] [PMID]
Review Paper: Applicable |
Subject:
Special
Received: 2021/12/20 | Accepted: 2022/06/11 | Published: 2022/07/1
Received: 2021/12/20 | Accepted: 2022/06/11 | Published: 2022/07/1
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Contact Information
Journal of Guilan University of Medical Sciences
Journal of Guilan University of Medical Sciences P.O. Box: 41938-93345, Iran
Tel/Fax: + (98-13)33330939
Email: medjour@gums.ac.ir
URL: http://www.Journals.gums.ac.ir
