

Volume 32, Issue 4 (1-2024)
JGUMS 2024, 32(4): 282-295 |
Back to browse issues page



Research code: IR.ABZUMS.REC.1399.252
Ethics code: IR.ABZUMS.REC.1399.252
![]()
![]()
![]()
Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
farahi Araghi F, Mortazavi S M, Esmaeili S, Esmaily M. Prevalence of Lip and Palate Clefts and the Related Factors in Babies Born From 2014 to 2019 in Karaj, Iran. JGUMS 2024; 32 (4) :282-295
URL: http://journal.gums.ac.ir/article-1-2505-en.html
URL: http://journal.gums.ac.ir/article-1-2505-en.html



1- School of Dentistry, Alborz University of Medical Sciences, Iran
2- Department of Oral and Maxillofacial Surgery, School of Dentistry, Alborz, Iran , drmo_mortazavi@yahoo.com
3- Department of Orthodontics, School of Dentistry, Alborz University of Medical Sciences, Iran
2- Department of Oral and Maxillofacial Surgery, School of Dentistry, Alborz, Iran , drmo_mortazavi@yahoo.com
3- Department of Orthodontics, School of Dentistry, Alborz University of Medical Sciences, Iran
Full-Text [PDF 3935 kb]
(99 Downloads)
| Abstract (HTML) (570 Views)
Full-Text: (113 Views)
Introduction
Congenital anomalies are a common cause of long-term disability in children, which has become an important medical issue [1]. Cleft lip (CL), cleft palate (CP), and cleft lip and palate (CLP) are common congenital anomalies. CP occurs in the secondary palate (soft and hard palate). Its occurrence may be unilateral, bilateral, complete, or incomplete. This abnormality can occur alone or along with CL or other syndromes [2]. The development of the lip and palate involves the events that need coordination; therefore, the occurrence of CL and CP is more common than the occurrence of each one alone. Veau et al. classified CL and CP into four main groups: soft palate cleft, hard palate cleft, unilateral CLP, and bilateral CLP [3].
Methods
This is a retrospective cross-sectional study on the data of babies born in Kamali, Imam Ali, Maryam, and Ghaem hospitals in Karaj, Iran, from March 2014 to February 2019. The sampling method was simple random method. The sample size was determined 3837 according to the study by Haseli et al. [17] who reported the ratio of CP as 0.001, and considering the accuracy of 0.001, which increased to 4000 by taking into account the possible dropout. In this regard, 1000 cases were selected from each hospital using a simple random method. The obtained data were analyzed in SPSS software version .24 using descriptive statistics (mean, standard deviation, frequency, and percentage) and chi-square test. P<0.05 was considered statistically significant.
Results
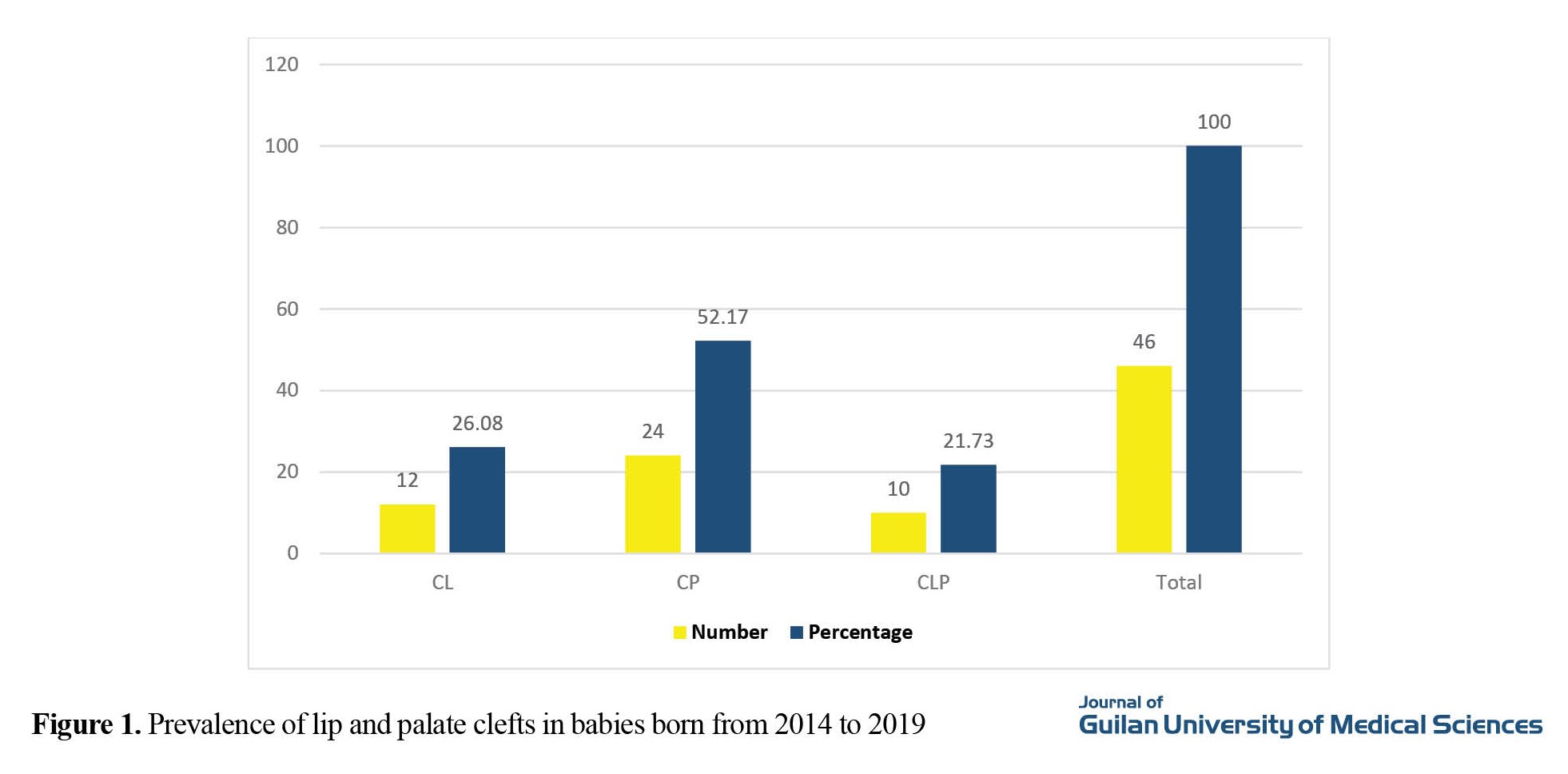
Of 91,563 live births, 46 had CL, CP, or CLP, with an overall prevalence of 0.5 per 1000 live births.
Out of 46 cases with clefts, 12(26.08%) had CL, 24(52.17%) had CP, and 10(21.73%) had CLP (Figure 1).
Congenital anomalies are a common cause of long-term disability in children, which has become an important medical issue [1]. Cleft lip (CL), cleft palate (CP), and cleft lip and palate (CLP) are common congenital anomalies. CP occurs in the secondary palate (soft and hard palate). Its occurrence may be unilateral, bilateral, complete, or incomplete. This abnormality can occur alone or along with CL or other syndromes [2]. The development of the lip and palate involves the events that need coordination; therefore, the occurrence of CL and CP is more common than the occurrence of each one alone. Veau et al. classified CL and CP into four main groups: soft palate cleft, hard palate cleft, unilateral CLP, and bilateral CLP [3].
Methods
This is a retrospective cross-sectional study on the data of babies born in Kamali, Imam Ali, Maryam, and Ghaem hospitals in Karaj, Iran, from March 2014 to February 2019. The sampling method was simple random method. The sample size was determined 3837 according to the study by Haseli et al. [17] who reported the ratio of CP as 0.001, and considering the accuracy of 0.001, which increased to 4000 by taking into account the possible dropout. In this regard, 1000 cases were selected from each hospital using a simple random method. The obtained data were analyzed in SPSS software version .24 using descriptive statistics (mean, standard deviation, frequency, and percentage) and chi-square test. P<0.05 was considered statistically significant.
Results
Of 91,563 live births, 46 had CL, CP, or CLP, with an overall prevalence of 0.5 per 1000 live births.
Out of 46 cases with clefts, 12(26.08%) had CL, 24(52.17%) had CP, and 10(21.73%) had CLP (Figure 1).
The chi-square test results showed a significant difference in the prevalence of clefts in terms of type, where CP had the highest prevalence.
Among mothers of newborns with clefts, 27(58.69%) had first pregnancy, 11(23.91%) second pregnancy, 6(13.04%) third pregnancy, and 2 (4.34%) fourth or more pregnancies. Regarding the gender of the newborns with clefts, 26(56.52%) were boys and 20(43.47%) were girls. Also, regarding the blood group of mothers of newborns with clefts, 36.95% had blood group A; 15.21%, blood group B;17.39%, blood group AB; and 30.43%, blood group O (Table 1).
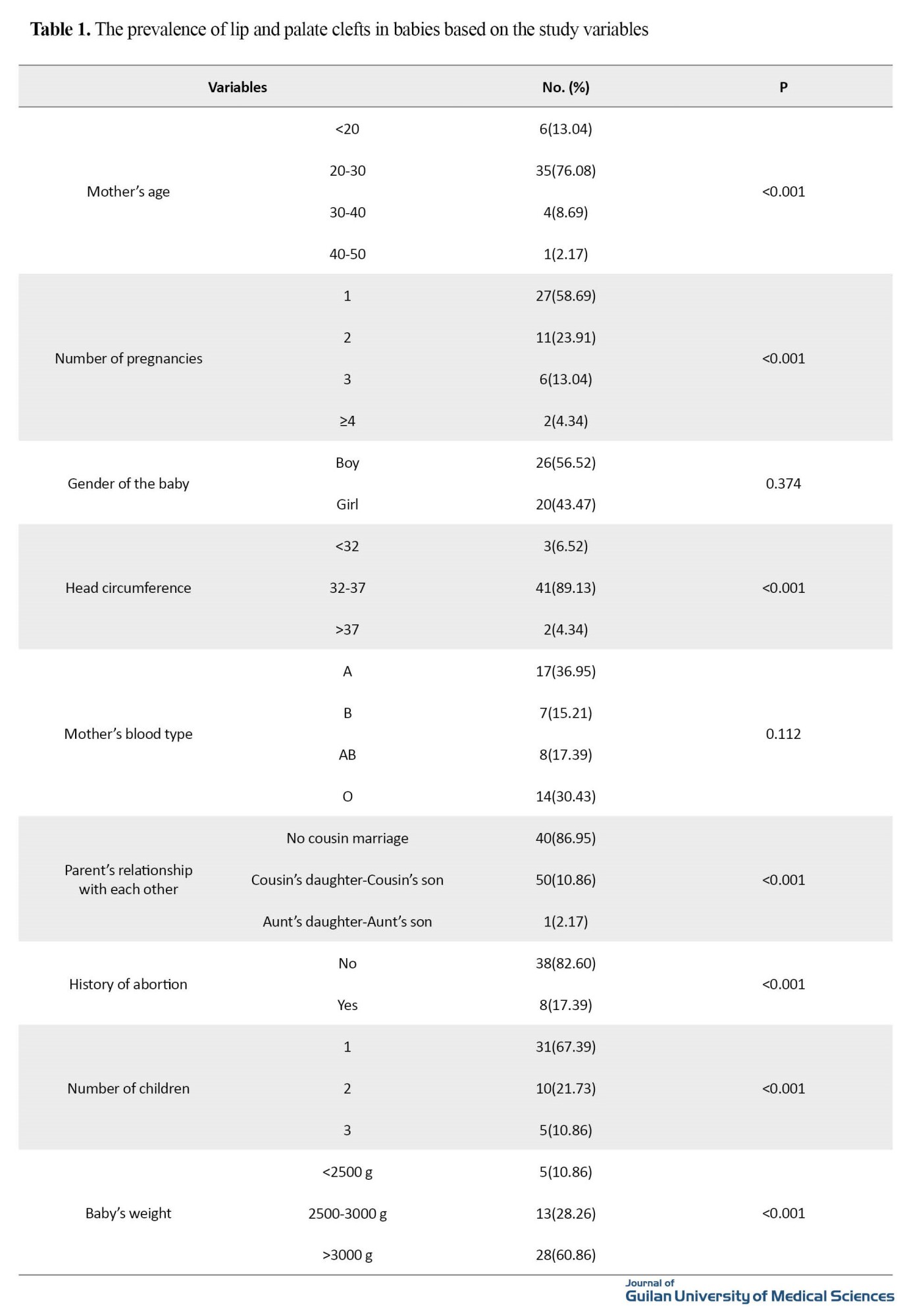
Three mothers had Rhesus (Rh) negative and the rest had Rh positive. None of the mothers had a history of alcohol or smoking. Only one mother had a history of opium use.
In assessing the number of children, 67.39% of mothers had one child, 21.73% had two children, and 10.86% had three children. A significant difference in the prevalence of clefts in terms of the number of children; the families with one child had the highest percentage of clefts. In assessing the weight of the baby, 10.86% had a weight <2500 g, 28.26% had a weight of 2500-3000 g, and 60.86% had a weight >3000 g. There was a significant difference in the prevalence of clefts in terms of infant weight, where babies above 3000 g experienced the highest percentage of clefts (Table 1).
Conclusion
Cleft lips and cleft palates are some of the congenital anomalies with low prevalence. These anomalies not only endanger the child’s health but also cause many economic, psychological and social problems for families. Identifying the factors related to the development of these anomalies can have a very important contribution to reducing the problems of families. Based on the results of this research, during a 5-year period from 2014 to 2019, 46 cases of clefts were recorded in 91,563 live births.
The overall prevalence was 0.5 per 1000 live births. This is lower than the prevalence reported by Ghafari et al. (2.22 per 1000 live births) and Kayanifar (1.9 per 1000 live births), Hasli (1.24 per 1000 live births), Namdar et al. (1.2 per 1000 live births) [13, 16, 17, 20], but is close to the reports of Jalilevand (0.485 per 1000 live births), Jahanbin (0.69 per 1000 live births) and Farhadian (0.83 per 1000 live births) [21-23].
In terms of the type of clefts, the highest prevalence was related to CP (52.17%), followed by CL (26.08%) and CLP ( 21.73%). In this study, the prevalence of clefts was higher in male babies, babies with mothers aged 20-30 years, babies with mothers having first pregnancy, babies with maternal blood group A, babies with parents having cousin marriage, babies with a head circumference of 32-37 cm and a weight of 2500-3000 g. To reduce the prevalence of clefts, it is recommended to increase the awareness of families to reduce cousin marriages and emphasize more on the use of complementary medicines for pregnant mothers.
Ethical Considerations
Compliance with ethical guidelines
The ethical approval of this study was obtained from the Research Ethics Committee of Alborz University of Medical Sciences (code: IR.ABZUMS.REC.1399.252).
Funding
This article was extracted from the thesis of Seyed Mostafa Mortazavi. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors' contributions
Conceptualization, design, drafting the manuscript, editing & review: Faraz Farahi Araghi; Acquisition and interpretation of data: All authors; Statistical analysis and supervision: Seyed Mostafa Mortazavi.
Conflicts of interest
The authors declare no conflict of interest.
Acknowledgments
The authors would like to thank the participants for their cooperation.
References
Among mothers of newborns with clefts, 27(58.69%) had first pregnancy, 11(23.91%) second pregnancy, 6(13.04%) third pregnancy, and 2 (4.34%) fourth or more pregnancies. Regarding the gender of the newborns with clefts, 26(56.52%) were boys and 20(43.47%) were girls. Also, regarding the blood group of mothers of newborns with clefts, 36.95% had blood group A; 15.21%, blood group B;17.39%, blood group AB; and 30.43%, blood group O (Table 1).
Three mothers had Rhesus (Rh) negative and the rest had Rh positive. None of the mothers had a history of alcohol or smoking. Only one mother had a history of opium use.
In assessing the number of children, 67.39% of mothers had one child, 21.73% had two children, and 10.86% had three children. A significant difference in the prevalence of clefts in terms of the number of children; the families with one child had the highest percentage of clefts. In assessing the weight of the baby, 10.86% had a weight <2500 g, 28.26% had a weight of 2500-3000 g, and 60.86% had a weight >3000 g. There was a significant difference in the prevalence of clefts in terms of infant weight, where babies above 3000 g experienced the highest percentage of clefts (Table 1).
Conclusion
Cleft lips and cleft palates are some of the congenital anomalies with low prevalence. These anomalies not only endanger the child’s health but also cause many economic, psychological and social problems for families. Identifying the factors related to the development of these anomalies can have a very important contribution to reducing the problems of families. Based on the results of this research, during a 5-year period from 2014 to 2019, 46 cases of clefts were recorded in 91,563 live births.
The overall prevalence was 0.5 per 1000 live births. This is lower than the prevalence reported by Ghafari et al. (2.22 per 1000 live births) and Kayanifar (1.9 per 1000 live births), Hasli (1.24 per 1000 live births), Namdar et al. (1.2 per 1000 live births) [13, 16, 17, 20], but is close to the reports of Jalilevand (0.485 per 1000 live births), Jahanbin (0.69 per 1000 live births) and Farhadian (0.83 per 1000 live births) [21-23].
In terms of the type of clefts, the highest prevalence was related to CP (52.17%), followed by CL (26.08%) and CLP ( 21.73%). In this study, the prevalence of clefts was higher in male babies, babies with mothers aged 20-30 years, babies with mothers having first pregnancy, babies with maternal blood group A, babies with parents having cousin marriage, babies with a head circumference of 32-37 cm and a weight of 2500-3000 g. To reduce the prevalence of clefts, it is recommended to increase the awareness of families to reduce cousin marriages and emphasize more on the use of complementary medicines for pregnant mothers.
Ethical Considerations
Compliance with ethical guidelines
The ethical approval of this study was obtained from the Research Ethics Committee of Alborz University of Medical Sciences (code: IR.ABZUMS.REC.1399.252).
Funding
This article was extracted from the thesis of Seyed Mostafa Mortazavi. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Authors' contributions
Conceptualization, design, drafting the manuscript, editing & review: Faraz Farahi Araghi; Acquisition and interpretation of data: All authors; Statistical analysis and supervision: Seyed Mostafa Mortazavi.
Conflicts of interest
The authors declare no conflict of interest.
Acknowledgments
The authors would like to thank the participants for their cooperation.
References
- Hebenstreit D, Pichler R, Heidegger I. Drug-drug interactions in prostate cancer treatment. Clinical Genitourinary Cancer. 2020; 18(2):e71-82. [DOI:10.1016/j.clgc.2019.05.016] [PMID]
- Rahnama F, Hasehmiyan M, Akbarzadeh R, Akabari A. [The incidence of apparent congenital anomalies in neonates in Mobini Maternity Hospital in Sabzevar Iran in 2005-6 (Persian)]. Journal of Sabzevar University of Medical Sciences. 2009; 15(4):231-6. [Link]
- Khosravifard N, Gholinia F, Ostovarrad F, Dalili Kajan Z, Mohammadi H, Farzam P. [Prevalence and type of dental abnormalities among patients with different skeletal malocclusion classes in Northern Iran (Persian)]. Journal of Guilan University of Medical Sciences. 2022; 31(4):300-11. [DOI:10.32598/JGUMS.31.3.1942.1]
- Abirami S, Panchanadikar NT, Muthu MS, Swaminathan K, Vignesh KC, Agarwal A, et al. Dental caries experience among children and adolescents with cleft lip and/or palate: An umbrella review. International Journal of Clinical Pediatric Dentistry. 2022; 15(Suppl 2):S261-8. [DOI:10.5005/jp-journals-10005-2169] [PMID]
- Boztepe H, Çınar S, Kanbay Y, Acımış B, Özgür F, Terzioglu F. Validity and reliability of the Family Empowerment Scale for parents of children with cleft lip and/or palate. Child: Care, Health and Development. 2022; 48(2):277-85. [DOI:10.1111/cch.12928] [PMID]
- Fan D, Wu S, Liu L, Xia Q, Tian G, Wang W, et al. Prevalence of non-syndromic orofacial clefts: Based on 15,094,978 Chinese perinatal infants. Oncotarget. 2018; 9(17):13981-90. [DOI:10.18632/oncotarget.24238] [PMID]
- IPDTOC Working Group. Prevalence at birth of cleft lip with or without cleft palate: Data from the International Perinatal Database of Typical Oral Clefts (IPDTOC). The Cleft Palate-Craniofacial Journal. 2011; 48(1):66-81. [DOI:10.1597/09-217] [PMID]
- Keuning KH, Wieneke GH, Dejonckere PH. The intrajudge reliability of the perceptual rating of cleft palate speech before and after pharyngeal flap surgery: The effect of judges and speech samples. The Cleft Palate-Craniofacial Journal. 1999; 36(4):328-33. [PMID]
- Doray B, Badila-Timbolschi D, Schaefer E, Fattori D, Monga B, Dott B, et al. [Epidemiology of orofacial clefts (1995-2006) in France (Congenital Malformations of Alsace Registry)(French)]. Archives de Pediatrie : Organe Officiel de la Societe Francaise de Pediatrie. 2012; 19(10):1021-9. [DOI:10.1016/j.arcped.2012.07.002] [PMID]
- Hupp JR. Contemporary oral and maxillofacial surgery. Missouri: Mosby Elsevier; 2008. [Link]
- Anai TA, Rajab MS, Mohammed SM, Jasem MF. Classification and identification of individuals using analysis lip prints. Tikrit Journal for Dental Sciences. 2022; 10(1):1-13. [Link]
- Koch H, Grzonka M, Koch J. Cleft malformation of lip, alveolus, hard and soft palate, and nose (LAHSN)-a critical view of the terminology, the diagnosis and gradation as a basis for documentation and therapy. British Journal of Oral and Maxillofacial Surgery. 1995; 33(1):51-8. [DOI:10.1016/0266-4356(95)90088-8] [PMID]
- Ghaffari HR, Poursamimi J, Keikhaie KR. [Evaluation of the prevalence rate of newborns with cleft lip and palate in the City of Zabol in 2018-2019 (Persian)]. Journal of Zabul Medical School. 2022; 119-25. [DOI:10.18502/jzms.v5i3.10923]
- Ghobadi N, Karami S. [A review of therapeutic approaches to cleft lip and cleft palate (Persian)]. Clinical Excellence. 2020; 9(3):35-42. [Link]
- Lowry RB, Trimble BK. Incidence rates for cleft lip and palate in British Columbia 1952-71 for North American Indian, Japanese, Chinese and total populations: Secular trends over twenty years. Teratology. 1977; 16(3):277-83. [DOI:10.1002/tera.1420160306] [PMID]
- Johnson N, Sandy J. Prenatal diagnosis of cleft lip and palate. The Cleft Palate-Craniofacial Journal. 2003; 40(2):186-9. [DOI:10.1597/1545-1569_2003_040_0186_pdocla_2.0.co_2] [PMID]
- Haseli A, Hajimirzaie S, Bagheri L, Sadeghian A, Ahmadnia E. [Prevalence of cleft lip and cleft palate in Iran: A systematic review and meta-analysis (Persian)]. Journal of Mazandaran University of Medical Sciences. 2019; 28(168):185-97. [Link]
- Fathololumi MR, Fattahi Bafghi A, Nuhi S, Nasiri Afshar AA, Aghazadeh Naieeni A. [Prevalence of cleft palate and cleft lip among 20000 Iranian neonates (Persian)]. Pajoohandeh. 2007; 12(1):31-4. [Link]
- Kianifar H, Hasanzadeh N, Jahanbin A, Ezzati A, Kianifar H. Cleft lip and palate: A 30-year epidemiologic study in North-East of Iran. Iranian Journal of Otorhinolaryngology. 2015; 27(78):35-41. [PMID]
- Namdar P, Etezadi T, Mousavi SJ, Maleknia A, Shiva A. [Frequency of cleft lip with or without cleft palate and related factors in a group of neonates in three hospitals in Sari, Iran, during 2004-2018 (Persian)]. Journal of Mashhad Dental School. 2021; 45(2):178-87. [Link]
- Jalilevand N, Jalaie S. Prevalence of cleft lip and palate among four provinces in the West and North-West of Iran. Journal of Research in Medical Sciences: The Official Journal of Isfahan University of Medical Sciences. 2015; 20(6):548-53. [DOI:10.4103/1735-1995.165951] [PMID]
- Jahanbin A, Kianifar H, Yaghoubi-Al Z, Malekian A, Keikhaee B, Hasanzadeh N, et al. Had prevalence of cleft lip and palate differed during the Iran-Iraq war? Journal of Craniofacial Surgery. 2013; 24(3):826-9. [DOI:10.1097/SCS.0b013e318290273d] [PMID]
- Farhadian N, Shahorkhi Z. Incidence rate and risk factors for cleft lip and palate hospital centres of Hamadan province, Iran in 2007. IIranian Journal of Orthodontics. 2013; 8(1):29-32. [Link]
- Azimi C, Karimian H. Cleft lip and cleft palate relationship with familial marriage: A study in 136 cases. Tehran University Medical Journal. 2010; 67(11):806-10. [Link]
- Khazaei M, Ghanbari S, Rezaei M, Alipour AA, Khazaei S. [Evaluation of cleft lip and palate frequency and related risk factors in infants born in Kermanshah Hospitals (2001-2008) (Persian)]. Journal of Isfahan Dental School. 2011; 6(4):298-304. Error! Hyperlink reference not valid.
- Silva RS, Macari S, Dos Santos TR, Werneck MAF, Pinto RDS. The panorama of cleft lip and palate live birth in Brazil: Follow-up of a 10-year period and inequalities in the health system. The Cleft Palate Craniofacial Journal. 2022; 59(12):1490-501. [DOI:10.1177/10556656211050004] [PMID]
Review Paper: Case report |
Subject:
Special
Received: 2022/05/30 | Accepted: 2023/01/30 | Published: 2023/12/31
Received: 2022/05/30 | Accepted: 2023/01/30 | Published: 2023/12/31
| Rights and permissions | |
 | This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |

Contact Information
Journal of Guilan University of Medical Sciences
Journal of Guilan University of Medical Sciences P.O. Box: 41938-93345, Iran
Tel/Fax: + (98-13)33330939
Email: medjour@gums.ac.ir
URL: http://www.Journals.gums.ac.ir
